
As a fitness professional you may encounter a situation where a client, colleague, or member of the public experiences a first-aid emergency and you will have to provide assistance until professional help arrives. The first aid situation may be at your workplace or it may be out in the general community.
Whilst you do not need to be a medical professional to administer first aid it is advisable that you are first aid accredited in both general first aid and CPR (note this topic and module are only providing an overview of the CPR component and therefore does not form a full first aid/CPR course).
The Australian Resuscitation Council (ARC) provides a series of guidelines related to the provision of first aid and managing emergencies. Their motto is:
Any attempt at resuscitation is better than no attempt
In Managing an Emergency (guideline 2) there are three key recommendations that rescuers should do to as part of the early management of an emergency situation:
-
Quickly assess the situation.
-
Ensure safety for the rescuer, person in need and bystanders (this may mean moving the person in need).
-
Send for help (call an ambulance).
These recommendations, along with further principles of patient management, are expanded and discussed in detail throughout the guideline.
The general principles of patient management (especially if the patient is unconscious, unresponsive, or not breathing normally) are:
-
Prevention of further harm or injury.
-
Checking response to verbal and tactile stimuli (talk and touch).
-
Care of airway and breathing (DRSABCD).
-
Control of breathing.
-
Checking for physical (eg. alert jewellery) or electronic alert devices (eg. smartphone app) that may be relevant to assessment or management.
-
Protection from the weather.
-
Other first aid measures depending on the circumstances.
-
Gentle handling.
-
Reassurance.
-
Continued observation.
Safe Work Australia, in conjunction with various States and Territories of Australia, has developed a model Code of Practice which includes information on first aid kits, procedures, facilities, and training for first aiders. This Code of Practice has been implemented in Queensland, New South Wales, Australian Capital Territory, Northern Territory and Tasmania. The remaining states have similar documents that they have developed independantly, see the below list/links:
According to Safe Work Australia's mode Code of Practice, people conducting a business have a duty to provide first aid services and facilities that are appropriate to their industry risk factor. For example, workers in factories, motor vehicle workshops and forestry operations are at a greater risk of injury requiring immediate medical treatment than workers in offices or libraries.
Therefore all business owners must write their Workplace, Health and Safety or First Aid Policy taking into consideration the following factors:
-
The nature of the work being carried out at the workplace.
-
The nature of the hazards at the workplace.
-
The size and location of the workplace.
-
The number and composition of the workers and other persons at the workplace.
To summarise the duty of care for employers is:
Business managers have the responsibility to comply with the Code of Practice, or other State regulated regulations, implement a workplace risk management program, and provide first aid services and facilities.
The DRSABCD process is a method of conducting a visual and verbal assessment of a patient and a means of initiating the chain of survival in the case of a sudden cardiac arrest and/or cessation of breathing incident.
The chain of survival principles in this context is:
-
Early Access - Recognising that the situation is a cardiac arrest/cessation of breathing incident and acting immediately to begin first aid treatment/resuscitation.
-
Early Cardiopulmonary Resuscitation (CPR) - If commenced within four minutes of the heart-stopping oxygenation of the vital organs can be maintained.
-
Early Defibrillation - Used in combination with CPR and within the 8-12 minutes of the heart-stopping, these devices can shock the heart back into action and restore correct rhythm.
-
Early Advanced Life Support - Medical treatment delivered by professional paramedics, nurses and doctors. An ambulance should ALWAYS be called in the case of a sudden cardiac arrest and/or cessation of breathing incident.
Ensure the area is safe for yourself, others, and the patient. Potential dangers include:
-
Electrical hazards after electrocution.
-
Traffic hazards after a car accident.
-
Fire or smoke hazards.
-
Wildlife hazards ie. snake, wasps etc...
-
Exposure to blood, vomit, and other bodily fluids (refer to infection control standard precautions later in this section).
It may not be possible to completely remove or eliminate a hazard, however, due caution should be taken and if absolutely necessary the casualty (patient) should be moved from the dangerous area.
Often a person experiencing a medical/first aid emergency will be unconscious or not fully responsive. To determine the level of response you must conduct a visual and verbal assessment of the patient. Squeeze their shoulder and ask them to open their eyes and/or say their name.
If they are conscious and responsive then some of the following steps (notably the airway, breathing, CPR and defibrillation steps) are not applicable, in that situation just make the patient comfortable and monitor them until further assistance arrives.
Most first aid emergencies will require some form of further medical treatment, in this situation you may need to call an ambulance (dial 000). If there are other people around then ask them to call the ambulance whilst you undertake the other steps in this process. If an ambulance has been called then ensure there is someone ready to meet them and guide them to where you and the patient are located, this is particularly important if you are located within a large building.
Airway management is required to provide an open airway when the person is unconscious, has an obstructed airway, or requires rescue breathing. Open the mouth, inspect for, and remove any foreign material, common items are:
-
Vomit.
-
False teeth.
-
Food.
-
Small objects that may have been swallowed.
The next step is to position the head for resuscitation. For adults and children above the age of one year, tilt the head back to fully open the airway. For infants (under one year of age) the head should be kept in a neutral position and maximum head tilt should NOT be used. If simple airway manoeuvres (chin lift) do not open the airway, then a slight backwards head tilt may be needed to open the airway.
The applicable Australian Resuscitation Council (ARC) guideline for Airway Management (Guideline 4) provides more specific information about this important aspect of the DRSABCD process.
Continue the visual and verbal assessment of the patient by checking for breathing using the Look, Listen and Feel method:
-
Look for movement of the upper abdomen or lower chest.
-
Listen for the escape of air from nose and mouth.
-
Feel for movement of air at the mouth and nose.
If the patient is breathing then place them in the recovery position, laying on their left side, and monitor their breathing until further assistance arrives. This position helps to maintain an open and clear airway by allowing for the drainage of body fluids, such as vomit, which may cause an additional choking hazard if the patient is in any other position.
The applicable Australian Resuscitation Council (ARC) guideline for Breathing (Guideline 5) provides more specific information about this important aspect of the DRSABCD process.
.png)
If the patient is not breathing and/or they have no detectable heartbeat then Cardiopulmonary Resuscitation (CPR) should be attempted. The two processes of CPR are chest compressions and mouth-to-mouth. Chest compressions are used to circulate blood around the body if the heart is not beating and therefore unable to do this vital task. Mouth-to-mouth is the transference of oxygen from you to the patient if they are not breathing. Instructions for these processes as per the Healthdirect.gov.au website are:
To carry out chest compressions:
-
Place the patient on their back and kneel beside them.
-
Place the heel of your hand on the lower half of the breastbone, in the centre of the person's chest. Place your other hand on top of the first hand and interlock your fingers. Note: If performing compressions on an infant (less than one year of age) use the two-finger technique to perform the compressions to minimise transfer time from compression to ventilation.
-
Position yourself above the patient's chest.
-
Using your body weight (not just your arms) and keeping your arms straight, press straight down on their chest by one-third of the chest depth (more than 5cm in adults, approximately 5cm in children and 4cm in infants).
-
Release the pressure. Pressing down and releasing in one compression. Aim for 100-120 compressions per minute (if only undertaking chest compressions).
-
If a second rescuer is available then ensure you rotate regularly (recommended every two minutes) to avoid exhaustion. Try to keep the interruption to CPR that occurs during rotation to an absolute minimum by having the second rescuer ready to take over immediately after you move aside.
To carry out mouth-to-mouth:
-
Open the person’s airway by placing one hand on the forehead or top of the head and your other hand under the chin to tilt the head back (do not tilt the head back if the patient is an infant).
-
Pinch the soft part of the nose closed with your index finger and thumb.
-
Open the person’s mouth with your thumb and fingers.
-
Take a breath and place your lips over the patient's mouth, ensuring a good seal.
-
Blow steadily into their mouth for about 1 second, watching for the chest to rise.
-
Following the breath, look at the patient’s chest and watch for the chest to fall. Listen and feel for signs that air is being expelled. Maintain the head tilt and chin lift position.
-
If their chest does not rise, check the mouth again and remove any obstructions. Make sure the head is tilted and chin lifted to open the airway. Check that yours and the patient’s mouth are sealed together and the nose is closed so that air cannot easily escape. Take another breath and repeat.
If both processes are required then chest compression will take priority, perform 30 compressions followed by two breaths (known as the 30:2 rule), aim for five sets of the 30:2 rule in about two minutes.
If the patient is a pregnant woman then it is advisable to apply some padding under her right buttock/hip to tilt the abdomen to the left and alleviate pressure on major blood vessels, however, ensure her shoulders are still flat on the ground.
CPR should be continued until any of the following conditions have been met:
-
The person responds or begins breathing normally.
-
It is impossible to continue (eg. exhaustion).
-
A health care professional arrives and takes over CPR.
-
A health care professional directs that CPR be ceased.
The applicable Australian Resuscitation Council (ARC) guidelines for Compressions (Guideline 6) and Cardiopulmonary Resuscitation (Guideline 8) provides more specific information about this important aspect of the DRSABCD process.
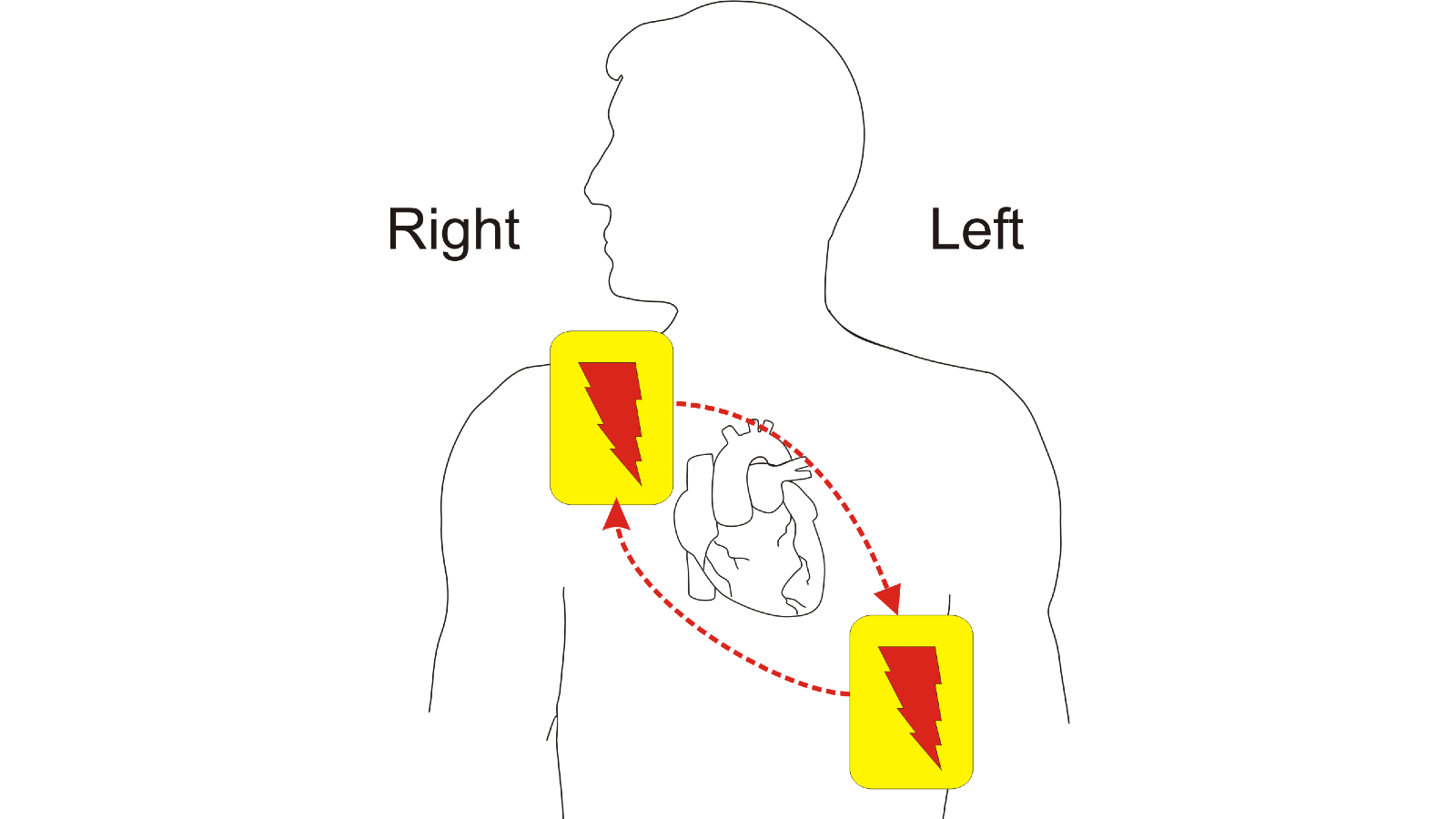
An Automated External Defibrillator (AED) is designed to provide electricity to re-start the heart or shock it back into its correct rhythm. If one is available then follow the instructions (audio which is spoken out loud) to place the pads in the correct place and start the process.
The pads are placed in the anterior (front) lateral (side) position of the body. This means one pad is placed on the persons right chest and one pad on the person's left side below the arm pit as shown in the image below:
Be prepared to continue CPR if the defibrillation doesn't work.
The applicable Australian Resuscitation Council (ARC) guideline for Defibrillation (Guideline 7) provides more specific information about this important aspect of the DRSABCD process.
Safe Work Australia have constructed a list of common hazards which may require first aid (note: this list is generic and does not apply specifically to the sport, fitness and recreation industry):
-
Manual tasks [Ergonomic] - Overexertion can cause muscular strain.
-
Working at height or on uneven or slippery surfaces - Slips, trips, and falls can cause fractures, bruises, lacerations, dislocations, and concussion.
-
Electricity - Potential ignition source - could cause injuries from fire. Exposure to live electrical wires can cause shock, burns, and cardiac arrest.
-
Machinery and equipment [Physical] - Being hit by moving vehicles, or being caught by moving parts of machinery can cause fractures, amputation, bruises, lacerations, and dislocations.
-
Hazardous chemicals - Toxic or corrosive chemicals may be inhaled or swallowed or may contact skin or eyes causing poisoning, chemical burns, and irritation. Flammable chemicals could result in injuries from fire or explosion.
-
Extreme temperatures - Hot surfaces and materials can cause burns. Working in extreme heat can cause heat-related illness. It can also increase risks by reducing concentration and increasing fatigue and chemical uptake into the body. Exposure to extreme cold can cause hypotermia and frostbite.
-
Radiation - Welding arc flashes, ionising radiation and lasers can cause burns. Ultraviolet (UV) radiation from the sun can cause sunburn, skin cancers and eye damage.
-
Violence - Behaviours including intimidation and physical assault can cause both physical and psychological injuries.
-
Biological - Infection, allergic reactions.
-
Animals - Bites, stings, kicks, crush injuries, scratches.
In addition to this generic list of hazards, the sport, fitness and recreation industry also has the additional hazard of health related incidents occurring as a result of clients will pre-existing medical or physical conditions overexerting themselves during fitness activities. This hazard can result in serious medical situations which require immediate first aid. Always ensure you have conducted the pre-exercise medical screening document developed by industry associations and provide adequate supervision.
When implementing a risk management program it is worth consulting this list to determine which of the hazards may be applicable to your workplace and formulating policies, procedures, and internal audit checklists accordingly.
Fitness Australia has developed a Fitness Industry Risk Management Manual which includes some first aid related risks among other generic risks that are applicable within the industry. They have identified the main areas of risk (not necessarily related to first aid) as being:
-
The competency of fitness professionals.
-
The effectiveness of pre-exercise screening and the management of de-conditioned clients.
-
Poor supervision of fitness service users and incorrect use of equipment.
-
Fitness trainers failing to remain within their scope of practice.
-
Equipment misuse (as distinct from incorrect use).
-
Poor fitness training environments.
Implementing safe work practices to minimise risk and potential hazards includes:
-
Identifying hazards - Find out what could cause harm.
-
Assess risks, if necessary - Understand the nature of the harm that could be caused by the hazard, how serious the harm could be and the likelihood of it happening.
-
Control risks - Implement the most effective control measure that is reasonably practicable in the circumstances and ensure it remains effective over time. This is known as the hierarchy of control, and it is discussed in more detail below.
-
Review hazards and control measures - To ensure they are working as planned.
The hierarchy of control methods can be used to help mitigate risks associated with hazardous activities or equipment.
-
Elimination - By completely removing a hazardous activitiy from a program or removing a dangerous piece of equipment from the facility the risk is eliminated. Although this may not be a practical solution.
-
Substitution - Replacing hazardous activities or equipment with a similar but safer alternative may be more practical than eliminating the situation altogether.
-
Engineering Controls - Making adjustments (or purchasing equipment with adjustments already installed) such as the inclusion of barriers, safety switches, or weight racks to alter a hazard to make it safer may be necessary.
-
Administration Controls - Implementing policies and procedures regarding hazards and risks to inform staff and clients of the hazard and risk and provide solutions on how to undertake safe work practices can be effective.
-
PPE - Providing personal protective equipment (PPE) and ensuring it is used when applicable, although this method should only be used in conjunction with at least one other method as it is not enough to mitigate risk all by itself.
Even with all of these safe work practices in place, first aid emergencies do still happen from time to time. Therefore managers and business owners should also be aware of the need for stress-management, counselling, and debriefing after a serious first aid incident. Staff members and bystanders, may be extremely distressed if they have had to deal with or have witnessed a traumatic event, especially a fatality.
Identifying a professional counselling organisation which might be able to visit the workplace and speak to staff is important. Debriefing can help in the following ways:
-
Provides participants with ways to deal with physical or psychological symptoms associated with trauma exposure.
-
Provides closure to the incident and sets in motion the rebuilding process.
-
Provides an opportunity to reflect upon the incident, and can provide valuable insight into existing policies and procedures and how they might be improved to prevent a recurrence.
Remember, people will have varying degrees of distress and therefore not everyone will want to participate (although it is highly recommended).
Infection control is an important consideration during the application of first aid to protect yourself and also the patient. M
Standard precautions that can be used to help promote infection control include:
-
Hand hygiene - Washing your hands prior to attempting first aid and wearing gloves (not applicable in emergency situations where urgency is required).
-
Using personal protective equipment (PPE) - Gloves, masks, eye protection, gowns and disposable face shields can all be used to prevent the transfer of body fluids.
-
Handling clinical waste (sharps, dressings, padding) appropriately - Disposing of clinical waste in specific biological waste cannisters is advisable.
-
Cleaning and managing spills of blood and body substances correctly - Appropriate cleaning products should be used to sanitise surfaces after a first aid incident, especially if blood and other body fluids were spilt. If necessary professional cleaning services should be contracted to correctly clean and dispose of contaminated surfaces and objects.
According to the Safe Work Australia Code of Practice the number of trained first aid officers employed in a workplace differs depending on the risk level of the business:
-
Low-risk workpalces - one first aider for every 50 workers (and/or clients).
-
High-risk workplaces - one first aider for every 25 workers (and/or clients).
-
Remote high-risk workplaces - one first aider for every 10 workers (and/or clients).
As the sport, fitness and recreation industry is so broad, and includes provision to members of the public in varying numbers, the risk factor would likely be high-risk for larger fitness facilities such as gyms or organised sport arenas. However, small operations such as community fitness or personal training may be considered low-risk if they do not service many clients at any one time.
Consideration should always be made regarding the specfic type of physical activity being undertaken and the percentage of clients that have been asssessed as moderate to high risk.
First aid accreditation is evidenced by a Statement of Attainment issued by a Registered Training Organisation (RTO) for the nationally endorsed unit of competency HLTAID003 Provide First Aid (and possibly also HLTAID001 Provide Cardiopulmonary Resuscitation). Industry recommendation is that HLTAID003 should be renewed every three years and HLTAID001 should be renewed every 12 months.
You must be aware of your own skills and limitations regarding first aid. If you do not feel confident in your skills and knowledge then consider the following tactics:
-
Undertaking a refresher course or perhaps and advanced training program.
-
Organising or participating in scenario drills at your workplace to ensure you and everyone knows how to handle first aid related incidents confidently.
-
Speak to your manager (if applicable) to ensure there are other first aid officers trained and on shift so you are not the only qualified person.
-
Consult workplace policies and procedures, as well as industry standards and codes of practice, for helpful strategies.
As part of establishing a first aid policy for your workplace/business due consideration must be made to protect the privacy and confidentiality of employees and clients. Things to consider include:
-
Discretion when discussing any medical conditions. This should be undertaken in a private room and records kept confidential and secure.
-
Consent should be obtained regarding the disclosure of any medical information to appropriate personnel (ie. ambulance officers) in the event of a first aid related emergency. This consent can be obtained verbally from the patient if they are conscious or it can be obtained in writing prior to activity ie. during the initial screening discussion / orientation.
-
First aid rooms should offer privacy in the form of screening or a door.
-
Where possible consent should be obtained prior to attempting first aid on a patient, if the patient is under 18 years of age then consent should be obtained from their parent or guardian. This consent may be obtained prior to undertaking an activity (especially a high-risk activity) and may be included in the membership contract wording. If the patient is unconscious then first aid consent is not required, although it may already be inferred through the prior consent process.
People who are ill or injured may be extremely distressed and require reassurance and information about their predicament, who you are, what you going to do, and how they can manage their own reactions (ie. breathing techniques). At all time respectful behaviour towards the patient is required.
